
Updated: 18 Feb 2021
The typical placement into a residency program occurs towards the end of medical school, via a computerized ranking system that considers both the prospective resident’s ranking of programs and the program’s ranking of those that have interviewed with it. This is “The Match.” After that initial match and the beginning of residency, if there is an interruption in training before the 3-5+ year residency program has been completed, the yet-to-be board certified physician needs to finish a program somewhere, in some specialty, in order to become board eligible (qualified and able to sit for the board certification exams). While one may typically obtain a medical license after one year of residency training (two years for foreign medical graduates) and be a “general practitioner (GP),” the options for practice and income are limited.
On this page, we will explore taking a path that diverges from the norm, whether that is finding another residency program, taking a year to “do research,” finding work as a GP, working as an Assistant Physician, or other.
How do you find a different residency program when the one you matched into is no longer a viable option? (e.g. it’s toxic, it’s closing, you’re terminated, you want to change fields,…)
Residency search for Open Training Positions:
Association of Residency Program Directors, e.g. the Association of Program Directors in Surgery (APDS)

This is a pay site. ?<$100 for 90 day access.
From their site: “Most comprehensive database of unfilled residency vacancies. In addition to openings that are posted directly on ResidentSwap.org, or reported by the members, ResidentSwap continually monitors over 50 websites that publicly advertise openings. This makes ResidentSwap the largest single database of residency vacancies.”
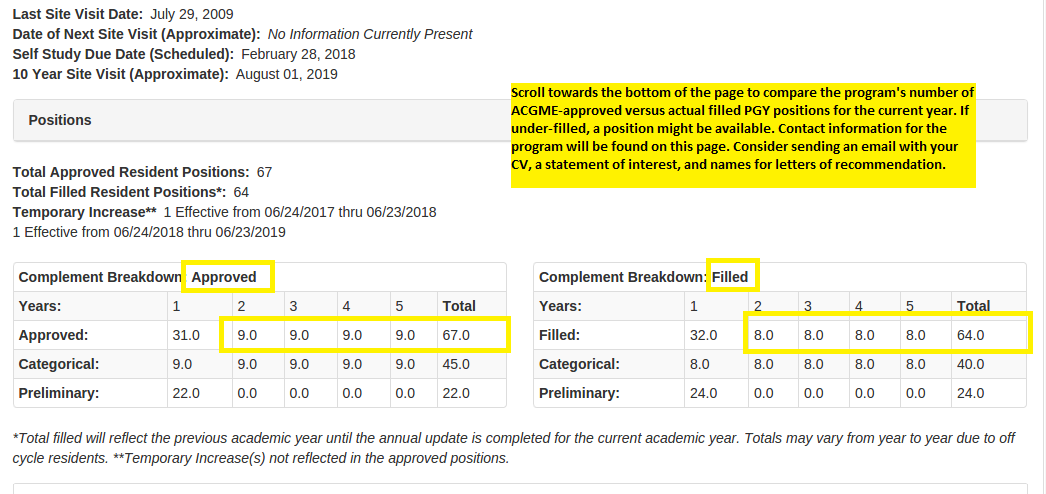
ACGME program search at the top of the home page – look for unfilled positions by specialty and program.



Consider Direct Primary Care (DPC). If you’ve completed a year of internship, you are eligible for a medical license in many states. In some states, two years of residency training are required.
You can practice as a generalist. If you are not board certified in a specialty, you may not be considered for hospital privileges or for insurance credentialing. However, you can run your own cash-based clinic and do very well. You do not even need any staff when starting out. Rent a space. Start with some scheduling and billing software. No insurance hassles or denials. If you charge $70 per patient per month, and keep a patient panel of 300 patients, with an overhead of under $2000 a month, you do the math. Help your patients find wholesale pricing for meds, diagnostics, x-rays. Learn to do some minor office procedures. Be available to your patients by text, email, phone. You can offer them significant value and end up saving them money when compared to their out-of-pocket expenses and deductibles.
Check out some of these links:
AtlasMD in Kansas City is one of the leaders in DPC.
DPC Frontier: “Defending Direct Primary Care, expanding the DPC Movement, Lowering barriers to entry into DPC for fellow physicians.”
Direct Primary Care Coalition: “Direct Primary Care (DPC) is an innovative alternative payment model improving access to high functioning healthcare with a simple, flat, affordable membership fee. No fee-for-service payments. No third party billing. The defining element of DPC is an enduring and trusting relationship between a patient and his or her primary care provider. Patients have extraordinary access to a physician of their choice, often for as little as $70 per month, and physicians are accountable first and foremost their patients. DPC is embraced by health policymakers on the left and right and creates happy patients and happy doctors all over the country!”
The American Association of Family Practice (AAFP) page on DPC.

Physician Side Gigs: “… over 26,000 verified physicians who are interested in pursuing passion projects or alternate income streams. It is intended to support physicians in these endeavors and create opportunities to network and seek advice. The group also regularly discusses jobs, business skills, financial topics, life in medicine, and physician burnout.”

The List of Physician Side Hustles by Passive Income M.D.
“Please note that this is a growing list as I come across new ideas and receive submissions as well. So check back often and feel free to submit your own ideas down below. If you’d like to talk about these topics in near real-time, feel free to join our newly formed private FB group.”
Assistant/Associate Physicians
What do you do if you can’t get into a residency at all – unable to “match” as apparently hundreds are unable to do, and thus unable to finish the one to two years (for FMGs) of residency required in order to acquire a state medical license to even work as a GP? <insert statistics, references>
Missouri is the first state to offer a clinical practice track to non-residency trained, medical school graduate physicians.
The Association of Medical Doctor Assistant Physicians

From their site: “An Assistant Physician (In some states called an Associate Physician) is a new breed of provider. These highly educated Doctors were specifically made to tackle the tasks of Primary Care in Medically Under Served Areas and work with a collaborating physician. They have completed medical school, are nationally ECFMG/ACGME Certified, and are a great asset to any hospital, clinic, or urgent care facility.”

Missouri State Medical Association statement on the Assistant Physician Law.
Excerpt: “Missouri’s Assistant Physician law, the first in the nation, allows medical school graduates who have passed the prescribed medical examinations and who have not entered into postgraduate residency training to serve as Assistant Physicians. The law took effect August 28, 2014, and rules were promulgated in early 2017.”
News coverage, Kansas City, Dec 2017.

Check out residencyrehab‘s page:

Additional points:
- If you meet the requirements to obtain a state medical license (e.g. you’ve completed a year or two of residency, USMLE/COMLEX exam steps completed,…), apply as early as possible. This can take many months, especially if you have a disciplinary or flawed history. You may have to appear before the medical board. You may need an attorney. Once you have a license, you can find an income generating opportunity.
- Work in anything health related as soon as you can. Medical boards and credentialing agencies note any gaps in your training/work history as red flags. Even if you volunteer in a clinic, do something to show continued engagement in Medicine, and also to keep your mind focused. Do research. Teach. Tutor. Even one day a month is something. The board/credentialing history question is something like: “have you ever had a 30-day or longer gap in your medical training or practice.” If you can’t avoid the gaps, make sure you can show related activity within those gaps.
- Be assertive in finding residency openings. Cold call/email programs with your interest. Make a spreadsheet to document with which programs/directors you’ve communicated. Have documents ready: CV, USMLE scores, In-Training Exam scores, personal statement, letters of reference, copy of medical school diploma, internship completion certificate (if applicable), a head shot photo,….
- We have spoken with physicians who were out of residency for up to 5 years before getting back in a position. Make yourself marketable. Study for the board exam in your down time. Improve whatever situation or condition that can/will be focused upon in an interview.
- If you believe you were victimized by your previous program/director, that is likely not a topic that is going to go over well with a potential future program. Due to bias, disbelief, an unprovable “he said, she said” situation, etc. it is likely to hurt your chances in acquiring a new program if your initial approach is to put blame elsewhere. Try to take as much blame for past failures as possible, be humble, state what you learned and will do differently. Your interviewer will want more details about your departure. Be cautious with criticisms – these people may know each other, may have already talked about you, and will almost certainly align their perspectives before they adopt yours. Find a way to be honest, but to share responsibility. A new program does not want a “problem resident.” Show them that you are emotionally mature, a hard worker, and just want to get the work and learning done in order to reach your goals. You are looking for a program that will facilitate that, and you have a lot to offer your new program in experience, initiative and work ethic.
Our Programs. Our Future. Our Responsibility.

GMECP: Driving education, awareness, and positive change towards systemic improvement for our programs’ residents, faculty, and staff.
⇑ to Top of Page
⇐ To Home Page
*Disclaimer: We are in no way associated with or supported by any educational, administrative, accreditation, licensing or oversight body mentioned in these pages.
*Legal: Institutional images and names are used non-commercially and under concepts of fair use, public domain, sharing of newsworthy and public-benefiting criticism, and with an unlikelihood of confusion as to trademark usage.